
Statins are one of the most prescribed heart medications, and among the most debated. In fact, millions of people take a statin daily to manage their cholesterol.
As a clinical pharmacist, I often hear patients ask: “Do I really need this medication, and if so, for how long?”
This article provides an evidence-based guide to statins and other major heart medications. We’ll cover what these drugs do, their benefits and risks, when they’re truly needed (and when they might not be), the basics of other common cardiovascular drugs, and how healthy lifestyle choices and nutrition play a vital role in heart health. My goal is to help you understand these treatments so you can make informed decisions about your care.
Why Are Statins and Other Heart Medications Prescribed?
Heart medications have one primary purpose: to reduce the risk of life-threatening problems like heart attacks and strokes. They aren’t prescribed just to improve “bad numbers” on a lab test. These drugs help control underlying risk factors such as high cholesterol, high blood pressure, or clotting, and slow the progression of heart and blood vessel disease.
Take statins as an example. Doctors don’t recommend a statin simply to lower your cholesterol for its own sake. The real goal is to lower your chance of a future heart attack or stroke. When deciding if a statin is right for you, doctors look at your overall cardiovascular risk profile. That means considering factors like your age, blood pressure, smoking status, blood sugar control, family history of heart disease, and any evidence of plaque buildup in your arteries - not just your cholesterol number! If those factors add up to moderate or high risk, adding a statin can provide a layer of protection that significantly reduces the likelihood of a heart attack or stroke.
Other heart medications are prescribed for similar reasons; each one addresses specific risk factors or heart problems to prevent bigger issues down the road. For example, someone who’s had a heart attack is often sent home on a combination of medications: typically a statin (to manage cholesterol and stabilize arterial plaques), a beta blocker (to reduce the heart’s workload), an ACE inhibitor (to lower blood pressure and protect the heart and kidneys), an antiplatelet medication and/or a low-dose aspirin (to prevent blood clots). Research shows that each of these medications can improve survival or reduce complications after a heart attack. In short, doctors use these drugs when the evidence shows the benefits (like preventing future heart events or helping the heart pump better) outweigh the risks for that patient.
Statins – How They Work & Their Benefits
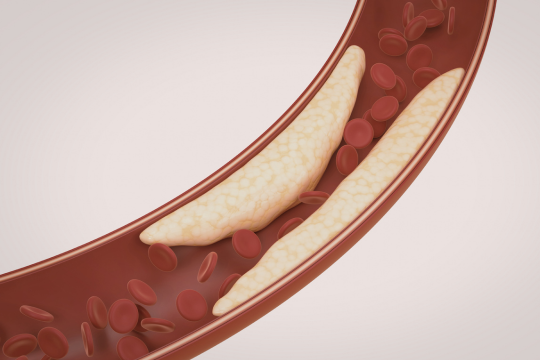
Statins reduce the liver’s production of cholesterol, especially lowering levels of LDL (the “bad” cholesterol). But their benefits go beyond just improving a lab number. Statins also reduce inflammation in blood vessels and stabilize fatty plaques that build up in arteries. This is crucial because many heart attacks and strokes occur when an inflamed plaque in an artery ruptures and forms a clot that blocks blood flow. By reducing inflammation and strengthening plaques, statins make these dangerous clots less likely to form.
How effective are statins?

In people with established heart disease – for example, those who have already had a heart attack or have significant artery blockages – statins are proven to lower the chance of another heart attack or stroke by roughly 20–30%. That’s why, if you have a history of cardiovascular disease, taking a statin long-term is considered a standard (and potentially lifesaving) part of your treatment.
Statins can also help prevent a first heart attack or stroke in people with risk factors (this is called primary prevention). The higher your overall risk, the more likely a statin will meaningfully lower it. If you have multiple risk factors like high blood pressure, high cholesterol, and a strong family history, a statin can significantly cut the likelihood of a future cardiovascular event. Health guidelines in North America suggest that many people in their 40s and beyond who have an elevated 10-year risk of cardiovascular disease should consider taking a statin daily.
On the other hand, if you’re a healthy person with only mildly elevated cholesterol and no other major risk factors, the benefit of a statin is only modest. In these cases, it’s often reasonable to focus on lifestyle improvements first and possibly hold off on medication. Statins are best used when your risk is high enough that the potential benefit, in terms of heart attack and stroke prevention, clearly outweighs the inconvenience or any side effects of taking a daily pill. With your healthcare provider’s help, you can determine if that’s the case for you.
Statin Side Effects – Separating Fact from Fiction
Most people take statins without serious problems. Many of the scary stories about side effects are exaggerated or don’t apply to the average patient.
- Muscle aches or fatigue: This is the side effect you hear about most, but only about 5-10% of people on statins experience it. Usually the discomfort is mild -perhaps some soreness or tiredness – and it often goes away with time or after adjusting the dose. Severe muscle damage from statins (such as the rare condition rhabdomyolysis) is extremely unlikely. You’re far more likely to pull a muscle from exercise than to have a muscle break down because of a statin.
- Blood sugar and diabetes: Statins can slightly raise blood sugar levels. In a small number of people, this might mean they develop type 2 diabetes a bit earlier than they otherwise would. Importantly, for most individuals who need a statin, the heart-protection benefits far outweigh this small extra risk. And if your blood sugar does go up, it can usually be managed with diet, exercise, or medication.
- Liver function: True liver complications from statins are very rare. Doctors might do a blood test for liver enzymes when you start a statin, but routine long-term liver monitoring isn’t needed unless you develop symptoms of a liver problem (like unusual fatigue or yellowing of the skin or eyes). For most people, the liver tolerates statins well.
- Memory concerns: There have been worries about memory loss or “brain fog” with statins, but extensive research hasn’t found clear evidence of significant cognitive problems in most people. A few individuals have reported mild, reversible memory issues, but these cases are uncommon. Overall, there’s no strong proof that statins cause memory decline or dementia.
- Other side effects: Mild nausea, stomach upset, or trouble sleeping can happen, but these are not very common. In fact, large trials comparing statins to placebo have found no significant difference in the overall rate of side effects between those taking statins and those not taking them – suggesting that many reported minor symptoms might not be caused by the statin at all.
The bottom line: Statins have a good safety profile for most users. Serious side effects are rare. If you do experience side effects or feel that a statin isn’t agreeing with you, talk to your healthcare provider rather than stopping the drug on your own. We have many strategies to help you stay on a beneficial medication: for example, lowering the dose, switching to a different statin (some people tolerate one better than another), or trying an alternate therapy if necessary. The goal is to protect your heart without hurting your overall quality of life.
When Do You Need a Statin – And When Might You Not?
Here are some general guidelines on who benefits most from statins and who may not need them:
When Are Statins Clearly Needed?
- After a heart attack, stroke, or diagnosis of heart disease. If you’ve already had a serious cardiovascular event or you have known clogged arteries, a statin is almost always recommended to help prevent further problems. This is often called “secondary prevention” (preventing another event).
- Very high LDL cholesterol. If your LDL (“bad” cholesterol) is extremely high (around 190 mg/dL or above), often due to genetic factors, a statin is strongly advised because your long-term risk of heart disease is very high.
- Diabetes (over 40 years old). Diabetes greatly increases your risk of heart attacks and strokes. Most people over 40 with diabetes are put on a statin to reduce that risk, even if their cholesterol isn’t extremely high.
- High overall risk. If your doctor determines that your chance of having a heart attack or stroke in the next 10 years is high (for example, above 20%), a statin can provide significant protection even if you haven’t had a heart event yet. In this scenario, the data show that the medication can substantially lower your risk.
When Might a Statin Not Be Necessary?
- If you’re low-risk. When your odds of a heart attack or stroke in the near future are very low, a statin might not offer enough benefit to justify taking a daily medication. In this case, focusing on healthy habits may be the better approach.
- If lifestyle changes haven’t been tried yet. If your cholesterol is only moderately high and you haven’t yet improved your diet, exercise routine, weight, or smoking status, doctors usually recommend trying those changes first. Lifestyle improvements can sometimes lower your cholesterol (and overall risk) enough that you may not need medication.
- If you’re an older adult without heart disease. For someone over 75 who has never had a heart attack or stroke, starting a new statin is a nuanced decision. Some healthy seniors might not need one – it really depends on individual health status and life expectancy. This is something to discuss with a doctor, weighing the potential benefits and risks.
- If you absolutely can’t tolerate statins. A very small number of people experience side effects with every statin they try. If you’re one of them, your doctor can consider other cholesterol-lowering options (like ezetimibe or newer injectables) or focus on managing your heart risk through non-medication means.
It’s wise to review with your doctor from time to time whether you should start a statin or, if you’re already on one, whether you still need it. If your risk factors improve significantly (for example, you lose weight, improve your diet, quit smoking, etc.) or if your health status changes, your treatment plan might be adjusted. And if a decision is made to stop a statin, it should be done under medical supervision, with a plan to monitor your cholesterol and overall health and to restart the medication if needed. The goal is to use medications judiciously: give them when they’re truly needed and try to scale back when they’re not.
Quick Overview of Other Common Heart Medications
Statins are just one tool for protecting your heart. Doctors often prescribe other medications to people who are at risk of heart problems or who have had a cardiovascular event. Here are a few other common ones and what they do:
- Beta Blockers: These drugs (like metoprolol, atenolol, and other medicines ending in “-olol”) slow down your heart rate and lower blood pressure. They’re a standard treatment after a heart attack and in heart failure because they reduce the heart’s workload and help the heart heal and pump more effectively. Beta blockers also treat high blood pressure, relieve chest pain (angina), and help control certain heart rhythm issues. Common side effects can include fatigue or low energy, feeling lightheaded (due to a slower heart rate and lower blood pressure), and sometimes colder hands or feet. It’s important not to stop a beta blocker suddenly; if you ever need to come off this medication, your doctor will taper it down gradually to prevent your heart rate and blood pressure from spiking.
- ACE Inhibitors (and ARBs): ACE inhibitors (such as ramipril, lisinopril) and their close relatives, ARBs (like valsartan, losartan), relax and widen blood vessels. This lowers blood pressure and makes it easier for the heart to pump blood forward. These medications are key treatments for high blood pressure, and they also improve survival in people with heart failure or those who’ve had a heart attack. In addition, they help protect the kidneys, which is why patients with diabetes or kidney disease often take them. A frequent side effect of ACE inhibitors is a persistent dry cough (harmless but annoying). If that happens, doctors will usually switch you to an ARB, which has similar benefits but typically doesn’t cause a cough. Other side effects can include dizziness (if your blood pressure gets too low) and, very rarely, a serious swelling reaction called angioedema. Overall, these drugs are very beneficial for many heart patients and are well tolerated by most people.
- Antiplatelet Drugs: This category includes low-dose aspirin and medications like clopidogrel (Plavix). They help prevent blood clots by making platelets (the blood’s clotting cells) less sticky. After a heart attack, stroke, or stent placement, these medications are often lifesaving – they significantly reduce the risk of a new clot causing another blockage. However, they also increase the risk of bleeding, such as stomach bleeding or easy bruising. For someone who has already had a heart attack or similar event, the benefit of preventing another far outweighs the bleeding risk, so an antiplatelet drug is usually recommended long-term (often for life). On the other hand, if you haven’t had a heart attack or stroke, using aspirin to prevent one is no longer automatic. Doctors now carefully weigh the pros and cons because even a “baby” aspirin can cause bleeding. If you’re at very high risk of a heart attack, an aspirin might be advised, but if you’re low risk, the downsides of an unnecessary daily aspirin could exceed the small potential benefit. The key side effect to remember with any antiplatelet medicine is an increased tendency to bleed.
Of course, there are other cardiovascular medications as well. Calcium channel blockers (like amlodipine) can lower blood pressure and help with angina (chest pain). Diuretics (water pills such as hydrochlorothiazide or furosemide) help control blood pressure and reduce fluid buildup in heart failure. Nitrates (like nitroglycerin) can relieve chest pain by widening blood vessels. And there are even newer drugs for specific conditions (for instance, SGLT2 inhibitors for heart failure and certain diabetes patients, or PCSK9 inhibitors for very high cholesterol). Each medication has its own role, benefits, and potential side effects.
If you’re ever unsure why you’re on a particular heart medicine, ask your healthcare provider to explain how it fits into your care. Knowing the purpose of each medication helps you take charge of your health and work as a team with your provider.
The Importance of Lifestyle: Nutrition & Habits
Medications are powerful, but so are the choices we make every day. In fact, healthy lifestyle changes can sometimes rival the effects of a pill. More often, they work together with your medications to keep your heart strong.
Diet
A heart-healthy diet is a great place to start. Fill your plate with vegetables, fruits, whole grains, lean proteins (like fish, beans, or lean poultry), and healthy fats from sources like olive oil, nuts, and avocados. Cut back on excess sugar, salt, and processed foods. This kind of diet helps lower blood pressure, improve cholesterol levels, and control blood sugar.
Studies of Mediterranean-style diets have even shown a significant reduction in heart attacks and strokes among people who follow these eating patterns. If you need to lose weight, even a 5–10% weight loss can lead to meaningful improvements in your blood pressure, blood sugar, and cholesterol.

Exercise
Regular physical activity is another cornerstone of heart health. Try to get about 150 minutes of moderate exercise per week (for example, a 30-minute brisk walk five days a week). Exercise strengthens your heart, improves circulation, raises your “good” HDL cholesterol, helps control weight, and is one of the best stress relievers there is. Combine that with adequate sleep (about 7–8 hours per night for most adults) and stress management techniques (like meditation, yoga, or relaxing hobbies), and you create a solid foundation for your heart’s well-being.
Supplements
What about supplements? Some can support heart health, but they should complement (not replace) standard medical care. For example:
- Omega-3 fatty acids (fish oil) can lower high triglycerides and have mild anti-inflammatory effects. You can get omega-3s by eating fatty fish (like salmon) or through supplements if your doctor recommends them.
- Coenzyme Q10 (CoQ10) is sometimes used to help with statin-related muscle aches; evidence from studies is mixed, but some patients feel it makes a difference, and it’s generally safe to try with a doctor’s approval.
- Also, maintaining good levels of vitamin D and magnesium is important for heart and muscle function – if you’re deficient in these, your healthcare provider might suggest supplementation.
Always discuss any supplement with your provider to ensure it’s appropriate and won’t interfere with your other treatments.
Final Thoughts
By combining the right medications when they’re needed with positive lifestyle changes, you’ll be doing the best possible thing for your heart. The aim isn’t to rely on pills alone, nor to avoid them at all costs – it’s to use every tool available wisely. With a personalized plan that includes nutritious eating, regular exercise, consistent sleep, stress reduction, and appropriate medications, you can greatly reduce your risk of heart disease and enjoy a long, healthy life!
Disclaimer: This summary is for educational purposes only and does not replace personalized medical advice. Always consult your healthcare provider about your individual health and before making any changes to your medications or lifestyle.
