If you are interested in learning more about testosterone replacement therapy for women, it is important that first you understand the physiological role testosterone plays in the body for females.
Just like estrogen and progesterone, testosterone levels vary throughout a woman’s lifetime and vary from woman to woman. The bioavailability of the hormone also influences how a woman might feel depending on her blood levels of testosterone. All of these factors are important to understand before considering testosterone replacement therapy.
How is testosterone produced in women?
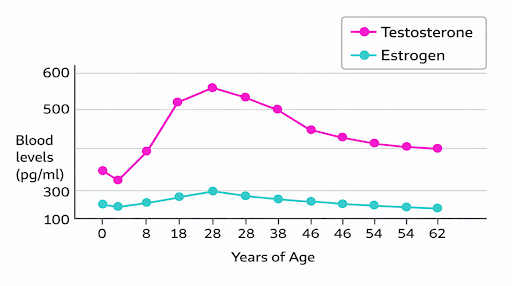
In women, testosterone is produced by both the ovaries and the adrenal glands. It is actually the most abundant sex hormone in women across the lifespan. Unlike estrogen and progesterone, testosterone continues to be produced by the ovaries even after menopause, although levels slowly decline with age (Figure 1). In addition to direct production, the body also makes testosterone from building-block hormones such as DHEA-S, DHEA, and androstenedione, which are produced mainly by the adrenal glands and ovaries and then converted into active hormones like testosterone and dihydrotestosterone (DHT) in tissues such as the skin and fat.
What influences testosterone levels in the body ?
Testosterone travels through the body acting on androgen receptors (AR). These receptors can be found in almost all tissues including the breast, heart, blood vessels, gastrointestinal tract, lung, brain, spinal cord, peripheral nerves, bladder, uterus, ovaries, endocrine glands, vaginal tissue, skin, bone, bone marrow, synovium, muscle and fat tissue. So, as you can see, testosterone plays a widespread role in the body.
Testosterone travels in the blood bound to a protein called Sex Hormone Binding Globulin (SHBG). The higher the amount of SHBG, the lower the amount of bioavailable free testosterone (because it binds it). This is how oral contraceptive pills help manage acne for young women, it increases levels of SHBG, lowering the amount of free testosterone in the blood. This results in less acne, but also lower libido, which is a well known side effect of the birth control pill.
Testosterone levels decline naturally throughout a woman’s lifetime, with a slight increase during perimenopause when there is a decline in SHBG levels. This is often when women might have a recurrence of adult acne due to higher circulating free testosterone levels (fun!).
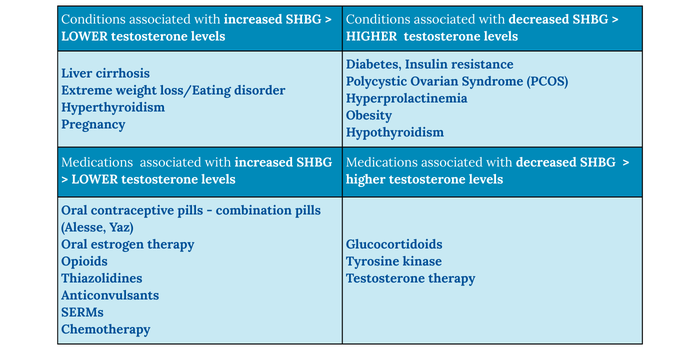
So, testosterone levels matter, but only in the context of the hormone that binds it (SHBG). Figure 2 depicts conditions such as diabetes, PCOS, hypothyroidism and obesity that are associated with lower SHBG levels, which are therefore associated with higher levels of free testosterone. In addition, certain medications can either increase or decrease the amount of free testosterone in the blood.
The bottom line is that testosterone levels are not the same in all women. The levels can vary throughout a woman’s hormonal transitions, with greater variances depending on health condition or medication use.
As previously mentioned above, testosterone has active receptors widespread throughout a woman’s body – so why is it that we think of testosterone for women only in the context of libido and sexual function? Testosterone is essential for women’s mental and physical well being.
What should my blood levels of testosterone be? Should I have my testosterone checked?
Normal testosterone ranges in women are wide, and lab cutoffs do not always match symptoms. How a woman feels reflects the balance between testosterone, estrogen, SHBG, and tissue sensitivity, not a single blood value.
In Ontario, testosterone levels for women are a range that are indicated to be “< 2.0 nmol/L” (see image below).For this reason, testosterone results should always be interpreted in the context of symptoms, life stage, and overall hormonal health, not as a standalone number.
How does testosterone influence female health?
Cognition & Mood
The brain is sensitive to changes in estrogen and testosterone, especially during menopause. Both of these hormones help protect the brain and reduce inflammation, and testosterone plays a role in memory, sleep, temperature control, and sexual desire. Some research suggests testosterone may help protect against brain aging by reducing harmful buildup in the brain and supporting nerve repair. Most women do not notice major thinking or memory changes during menopause, but some do, especially younger women who have had their ovaries removed. Overall, studies show that testosterone therapy does not harm cognition or mood, and some evidence suggests it may slightly improve certain types of memory.
Sexual Function & Libido
Testosterone plays an important role in libido and sexual function in women by supporting sexual desire, arousal, and pleasure. Testosterone acts on androgen receptors in the brain and genital tissues, helping increase sexual motivation, sensitivity, and responsiveness. Low testosterone levels have been linked to low sexual desire, reduced arousal, and decreased sexual satisfaction.
Sleep quality
Testosterone plays a supportive role in sleep quality by helping regulate circadian rhythm, sleep depth, and overall sleep efficiency. Normal testosterone levels are associated with better deep (slow-wave) sleep, which is important for physical recovery, mood, and cognitive function. Low testosterone may be linked with lighter, more fragmented sleep and increased fatigue. Poor sleep can also lower testosterone levels, creating a bidirectional cycle where sleep and hormones affect each other.
Muscle & Bone Health
Bone cells have receptors for testosterone, and low testosterone levels in women have been linked to lower bone density and a higher risk of fractures. Higher natural testosterone levels in postmenopausal women are linked with a lower risk of hip fractures, but there is not enough strong evidence to recommend testosterone therapy for bone protection. Some studies show that testosterone can increase muscle mass and strength, especially at higher-than-normal doses.
Cardiometabolic Health
Sex hormones like estrogen and testosterone affect the heart and blood vessels, but we are still learning exactly how. At normal levels, testosterone can help blood vessels relax and support healthy blood flow, but very high levels can cause blood vessels to tighten. Low testosterone has been linked with worse heart health, while estrogen seems to protect the heart. Studies in postmenopausal women show that having more testosterone compared to estrogen is linked to a higher risk of heart disease and heart failure. Most short-term studies suggest testosterone therapy is safe for the heart when levels stay in the normal range, but oral testosterone may worsen cholesterol, and long-term safety data especially in women who are at higher risk of cardiovascular disease is limited.
Skin & Hair
Testosterone can be converted by the enzyme 5-alpha-reductase into dihydrotestosterone (DHT), a potent androgen that strongly affects hair follicles. On the scalp, DHT causes hair follicles to shrink and shortens the anagen (growth) phase, leading to thinning and female-pattern hair loss. In contrast, DHT activation at the chin, cheeks, and upper lip can cause coarse hair growth, known as hirutism. Some women experience these effects even with normal blood testosterone levels due to higher local 5-alpha-reductase activity or increased follicle sensitivity to DHT. For example, women with female-pattern hair loss may use a drug called finasteride to block the enzyme 5-alpha-reductase and reduce DHT, reducing hair loss. In women with PCOS, higher ovarian testosterone production can further increase DHT levels, contributing to scalp hair thinning, unwanted facial hair, and acne.
Breast & Endometrial Tissue
Testosterone can be converted into estrogen in breast tissue, which raises theoretical concerns for breast cancer risk, but lab and animal studies suggest testosterone actually slows breast cell growth and may protect breast health. Reviews of studies show that testosterone therapy does not increase breast density or cause breast pain or lumps. Short-term studies have also not linked testosterone use to breast cancer. In a large study following women for several years, breast cancer rates in those using testosterone were similar to what is normally seen in the general population. At normal doses, testosterone therapy also appears to have very low risk to the uterus and endometrial tissue with no signs of abnormal tissue growth.
Key Takeaways
Testosterone is not a “male hormone” in women, it is an essential, lifelong hormone that influences brain function, sexual health, sleep, muscle and bone strength, cardiometabolic health, and skin and hair integrity. Its effects depend not only on total blood levels, but also on SHBG, tissue conversion, receptor sensitivity, and a woman’s overall hormonal environment. Because testosterone acts throughout the body, changes in its levels can have wide-ranging and sometimes unexpected effects, especially during perimenopause and menopause. Understanding this physiology is critical before considering testosterone replacement therapy.
Stay tuned for Part 2 of this series, where we will explore when testosterone therapy may be appropriate in menopause, how it is prescribed, and clinical pearls.
Ready for Personalized Hormone Support?
References
- Davis, S. R., Baber, R., Panay, N., Bitzer, J., Perez, S. C., Islam, R. M., … Wierman, M. E. (2019). Global consensus position statement on the use of testosterone therapy for women. Journal of Clinical Endocrinology & Metabolism, 104(10), 4660–4666. https://doi.org/10.1210/jc.2019-01603; PMCID: PMC6821450 (PubMed Central)
- Al-Imari, L. H. B. S., & Wolfman, W. L. (2016). The safety of testosterone therapy in women. Journal of Obstetrics and Gynaecology Canada. https://www.jogc.com/article/S1701-2163(16)35385-3/fulltext (Note: accessed full text via journal site) (jogc.com)
- Uloko, M., Rahman, F., Puri, L. I., & Rubin, R. S. (2022). The clinical management of testosterone replacement therapy in postmenopausal women with hypoactive sexual desire disorder: A review. International Journal of Impotence Research, 34(7), 635–641. https://doi.org/10.1038/s41443-022-00613-0 (PubMed)
- Glaser, R., & Dimitrakakis, C. (2013). Testosterone therapy in women: Myths and misconceptions. Maturitas, 74(3), 230–234. https://doi.org/10.1016/j.maturitas.2013.01.003 (jogc.com)
- The North American Menopause Society. (2024). The NAMS position statement on hormone therapy misinformation. https://menopause.org/wp-content/uploads/2024/09/TMS-statement-on-HT-Misinformation.pdf
- (2020). Prescribing testosterone and DHEA: The role of androgens in women. PubMed. https://pubmed.ncbi.nlm.nih.gov/33384313/ (PubMed)
- Smith, J. (2026). Trials and tribulations of testosterone therapy in women: Importance of sexual health nomenclature and evidence-based use. Cleveland Clinic Journal of Medicine, 88(1), 35–??. https://www.ccjm.org/content/88/1/35.long (Cleveland Clinic Journal of Medicine)
